|
|
Bulletin of Applied Computing and Information Technology |
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||
Integrating RFID Technology into a Drug Administration System |
|
03:01 |
|||||||||||||||||||||||||||||||||||||||||||||||
|
Bryan Houliston Houliston,B. (2005, May), Integrating RFID Technology into a Drug Administration System. Bulletin of Applied Computing and Information Technology Vol. 3, Issue 1. ISSN 1176-4120. Retrieved from ABSTRACTErrors in the administration of drugs to patients, along with other types of adverse drug events (ADEs), have proven to be very costly to the healthcare sector. One commonly proposed solution to the problem is the use of barcodes to uniquely identify both patients and drugs. The size of the ADE problem, and the success of a limited number of barcode-based systems, has prompted US healthcare regulators to endorse, or even mandate, their use. However, it has been suggested that limitations of barcodes adversely affect the usability of such systems, and that RFID technology offers a more suitable alternative. This paper documents the design and development of an extension to an existing barcode-based anaesthetic drug identification system, IDAS, which would allow it to functionally replace barcodes with RFID technology. The design is informed by a review of RFID application case studies, experiments with RFID hardware, and observation and interviews of anaesthetists. A demonstration of the prototype system suggests that RFID technology could functionally replace barcodes, but significant issues remain to be addressed. KeywordsRFID, barcode, drug administration 1. INTRODUCTIONInjuries to patients as a result of errors in administering drugs are known in the healthcare sector as adverse drug events (ADEs). ADEs have proven to be very costly in terms of both human life and scarce healthcare resources. Bates, Cullen and Laird (1995) find that 7% of patients admitted to US hospitals experience an ADE. Wilson et al (1995) report that 8% of ADEs in Australian hospitals are fatal and 17% result in permanent disability. Recent research from New Zealand (Davis et al., 2003) suggests around 2% of hospital admissions result in an ADE, with 12% of these resulting in death or permanent disability. Johnson and Bootman (1995) estimate that ADEs cost the US healthcare sector around US$80 billion annually. Such figures have prompted regulatory bodies and patient safety lobby groups to call for the increased use of information systems (IS) that address the causes of ADEs. Electronic databases of drug trial results and known drug interactions can reduce the chances of doctors ordering inappropriate medications. Computerised Physician Order Entry (CPOE) systems are intended to ensure that a doctors orders can be understood by other doctors, nurses and pharmacists (Berger & Kichak, 2004). In pharmacies, robots can eliminate errors in dispensing drug doses (Brooks, 2003). Bar Code Medication Administration (BCMA) systems use barcodes to uniquely identify patients and drugs, reducing the risk that patients are given the wrong medication (Patterson, Cook, & Render, 2002). Clinical studies suggest that BCMA systems might prevent up to 58% of ADEs (Anderson, Jay, Anderson, & Hunt, 2002, 2003; Jensen, Merry, Webster, Weller, & Larsson, 2004; Patterson et al., 2002). Yet very few healthcare organisations have implemented them. Recent market research by healthcare IS vendor Exavera Technologies (Collins, 2004c) suggests that in the US it may be as little as 2% of the countrys 64,000 hospitals. However, this seems likely to change in the near future. The US Food and Drug Administration (FDA) recently mandated that all drugs supplied to hospitals must include barcodes on their packaging (Food & Drug Administration, 2004). The US Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has issued guidelines on the use of barcodes for unique identification of patients (Joint Commission on Accreditation of Healthcare Organisations, 2004). The leading proponents of BCMA in New Zealand include Merry, Webster and their colleagues from the University of Aucklands Faculty of Medical and Health Sciences, Anaesthesiology Department. Barcoded drugs play a central role in their Injectable Drug Administration and Automated Anaesthetic Record System (IDAS) (Merry, Webster, & Mathew, 2001). Simulated operations and clinical trials comparing IDAS with traditional methods for administering anaesthetic drugs suggest that IDAS reduces the incidence of ADEs (Merry, Webster, Weller, Henderson, & Robinson, 2002; Webster, Merry, Gander, & Mann, 2004). However, they also identify some limitations of barcodes that may reduce the effectiveness of IDAS. More recently Merry and Webster have suggested radio frequency identification (RFID) technology as an alternative that addresses some of these issues (Merry & Webster, 2004). This paper describes a constructivist research project undertaken to determine whether RFID technology can functionally replace barcodes in IDAS. Section 2 describes IDAS and the usability problems identified during simulated operations. Section 3 briefly discusses the research methodology and the specific goals of the project. Section 4 documents the design and development of a prototype RFID-enabled IDAS. Section 5 highlights outstanding issues. Finally, section 6 presents conclusions. 2. THE IDAS SYSTEMSeveral hospitals in Auckland are using IDAS to support the administration of anaesthetic drugs during operations. The system has been designed based on first principles of patient safety. It provides procedures and tools for keeping the anaesthetic work area organised, for confirming drugs before administration, and for keeping a record of drugs administered.
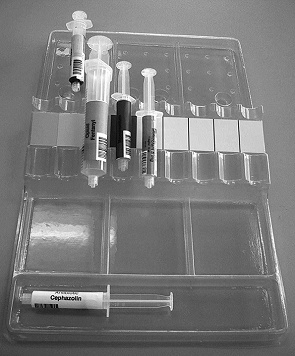
As illustrated in Figure 1, during an operation an anaesthetist spends most of their time within a triangular area defined by one or more drug trolleys, an anaesthetic workstation and the patient. Injectable drugs, some in ampoules and some in pre-filled syringes, are stored in the drug trolley. Under the IDAS system, the ampoules and syringes have a label attached showing the drugs class, name, and a barcode representing the Drug Identification Number (DIN). As shown in Figure 2, the label is also colour-coded based on the drugs class according to an international standard (Standards New Zealand, 1996). The top of the drug trolley is used as a work surface, on which the anaesthetist prepares injectable drugs for the operation. Drugs kept in ampoules are drawn up into syringes, which then have a corresponding barcode label attached. Under the IDAS system, plastic trays are used to keep the drug trolley drawers and work surface organised. An example of the trays used on the work surface is shown in Figure 3.
The anaesthetist controls infused drugs and monitors the patients condition via the anaesthetic workstation, shown in Figure 4. Pulse, blood pressure, and other vital signs are displayed on one monitor. A second monitor displays the IDAS software. This software allows an anaesthetist to use a keyboard to access details on the operation and the patient, and to monitor the patients fluid balance, and the drugs administered. Drug injections are recorded by scanning the syringes barcode label. This causes the IDAS software to display the name of the drug, and speak it aloud, providing the anaesthetist with confirmation that they are about to administer the intended drug. If the barcode label can not be scanned, then the keyboard can be used to select it from a drop-down list. Drugs are typically administered via an injection port at the patients neck or forearm. This reduces the risks inherent in repeatedly injecting directly into the patients body. The IDAS system has been compared with traditional anaesthetic practice through simulated operations (Merry et al., 2002; Webster et al., 2004). These have found that, while the IDAS system seems to reduce the incidence of ADEs, its effectiveness may be limited by usability issues. The major problem is anaesthetists administering a syringe without first scanning the barcode label. Half of the trial participants did this on at least one occasion. Comments from the participants suggest that this was mainly due to simple memory lapses. However, some comments were more directly related to the usability of the barcode scanner. For instance, one participant didnt use the scanner because of technical difficulties. Although it wasnt mentioned by participants in the trials, there is also reason to believe that some anaesthetists may regard the use of the scanner as a distraction. Barcode scanners can be inconvenient to use because they require a line-of-sight to the barcode label. As Figure 4 illustrates, the barcode scanner used in the trials was a simple hand-held model. These require more effort from an operator than the bi-optic scanners common in supermarkets. The anaesthetist must hold a syringe in a certain way for it to be scanned. The anaesthetist must move the syringe directly over the barcode scanner on the anaesthetic workstation, which may not be on the natural movement path from the drug trolley to the patient. The anaesthetist must pause at the barcode scanner long enough for the barcode to be recognised. The problem of unnatural movement may be exacerbated in some cases by anaesthetists who regard the scanner as an unwelcome big brother. Chassin (1998) finds that doctors are conditioned by their medical training to be self-reliant and to reject support systems. IDAS is a support system that requires extra effort from the anaesthetist, and which regularly reminds them that it is double-checking their actions. This is illustrated in the reaction of one trial participant, who initially did use the scanner but quickly stopped, finding it disconcerting to have the name of the drug spoken aloud. RFID technology offers solutions to some of these problems. RFID readers can sense RFID tags anywhere within range, even if they are obscured or moving. This allows the anaesthetist to hold the syringe in a natural way. While the tagged syringe must be moved somewhere near the RFID reader, it doesnt need to be paused at a specific location. This allows for more natural movement. 3. RESEARCH METHODOLOGYAfter reading of Merry et als interest in RFID, the researcher approached them with a proposal for a research project to determine whether RFID technology could functionally replace barcodes in the IDAS system. A constructivist methodology was suggested as most suitable for this research. Cornford and Smithson (1996, pg 44) characterise constructivist research as: concerned with developing frameworks, refining concepts or pursuing technical developments. In particular, practical hands on computing might be seen as within this broad area in that the aim is to create something and make it work, rather than to observe an existing system working or theorize as to cause and effect. Nunamaker, Chen and Purdin (1991) acknowledge that the research value of system development has been questioned. However, they go on to argue that it is a legitimate methodology for IS research. To ensure value from such research, Nunamaker et al propose an iterative multi-methodological approach. Theory building informs the development of prototype systems. These are evaluated through observation and experimentation, with the results informing a new cycle of theory building. The short time available for this research meant that only the first part of this cycle would be possible. Theory building was based on a review of RFID application case studies, experiments with RFID hardware, and observing and interviewing anaesthetists. This informed the development of a prototype system. In order to show that RFID technology could functionally replace barcodes in IDAS, this prototype was required to allow the following actions:
4. RESULTSCase studies of RFID applications were reviewed to determine which type of RFID tags and readers would be most suitable for use within the Anaesthetic Triangle. Experiments were then conducted to find out how different methods of attaching tags to syringes affected their performance. Anaesthetists were observed during an operation and interviewed to determine how RFID readers could best be deployed to fulfil requirement 3. Two small software tools were developed to perform requirements 2 and 4. 4.1 Selecting RFID HardwareThere is a small but growing body of case studies describing RFID applications in hospitals. The applications can be broadly classified into three types. Identification applications involve a single action at a single location. Identifying a staff member for access to a secure area is one example. Location-based applications perform continuous actions at a single location. For instance, an RFID-enabled smart medicine cabinet can provide a real-time inventory of the drugs it contains, recording removals and additions (Collins, 2004a). Tracking applications use continuous actions at multiple locations. For instance, individual pieces of equipment may be tracked to prevent them being lost or stolen (Broder, 2004), or staff and patients may be tracked to analyse workflow (Anonymous, 2003). The case studies reviewed show that almost all of these applications use RFID tags and readers that operate at either 13.56 Mhz or the 900-915 MHz band. These are the two frequencies most widely endorsed in RFID-related standards. This makes them popular choices for RFID manufacturers, ensuring that there should be a steady supply at a reasonable cost. Pappu, Singhal and Zoghi (2004) suggest that the 13.56 Mhz frequency is more common in identification and location applications, with 900 MHz typical in tracking applications. This reflects the different read ranges of the two frequencies. 900 MHz readers can detect a tag over several metres, while 13.56 MHz readers typically have a range of one metre or less. The Anaesthetic Triangle only covers a couple of square meters, so the latter should be more suitable. Another factor that differs between RFID frequencies is how the radio signals sent from the reader to the tag are affected by intervening objects. Walker et al (2003) point out that 13.56 MHz signals can be blocked or distorted by metal, and 900 MHz signals are absorbed by liquids. While there may be some metal objects such as surgical instruments in the anaesthetic work area, the RFID tags in this application will always need to be read through syringes filled with liquid. Based on this, it was decided that the prototype system would use 13.56 MHz RFID hardware. 4.2 Attaching an RFID Tag to a SyringeExperiments were carried out to determine how the tags should be attached to syringes. The aim was to find the method that resulted in the longest read range, while still allowing the anaesthetist to handle the syringe comfortably. The three most common sizes of syringe were used: 60 mls (approximately 30 mm in diameter and 110 mm long), 10 mls (16 mm diameter, 80 mm long) and 5 mls (13 mm diameter, 60 mm long). Three sizes of RFID tag were used: 80 x 50 mm, 50 x 50 mm and 40 x 25 mm. The larger the exposed area of an RFID tag, the more easily it can be read. A larger tag can be read at a greater range than a smaller tag, and tag laid flat at a greater range than a folded or bent tag (Chen & Thomas, 2001; Foster & Burberry, 1999). The maximum read range would therefore be provided by attaching the 50 mm edge of the largest tag to the syringe, with the rest of the tag protruding out from the syringe. Such large protrusions, however, would be impractical when placing syringes in close proximity on a syringe tray. In addition, anaesthetists suggested that having the RFID tag wrapped around the syringe would be preferable. When using IDAS they currently have to tent barcode labels to use them on smaller syringes. The label is folded in half so that the printed barcode is flat enough to be scanned, and attached so that the barcode itself protrudes around 10 mm from the syringe. Even this relatively small protrusion can cause handling difficulties. Table 1 shows the maximum read range of the smallest and largest tags attached by various means to the three sizes of syringe. Results for the 50 x 50 mm tag are excluded as they fall predictably in between. The results show that the smallest tag could be read as easily as the largest tag when wrapped around a large syringe, and more easily when wrapped around medium and small syringes. These results led to the decision that the prototype system would use 40 x 25 mm tags wrapped around syringes.
4.3 Reading an RFID TagIn the IDAS trials the barcode scanner was placed on the anaesthetic workstation. As already noted, this required the anaesthetists to pause while moving from the drug trolley to the patient. A few participants reduced this inconvenience by moving the barcode scanner on to the end of the operating table (Webster, 2004). This suggests that a more natural movement from drug trolley to patient would be facilitated by locating RFID readers at one, or both, these endpoints. As only a single reader was available for this prototype, one location had to be chosen. Both have strengths and weaknesses as the location for a reader. An RFID reader located on the drug trolley would detect when a tagged syringe has been removed. This is the earliest opportunity for the anaesthetist to be warned that they have selected the wrong drug, allowing them to correct error with the least effort. However, some anaesthetists keep syringes in places other than the drug trolley, so a reader there would not necessarily detect all syringes. Locating an RFID reader at the patient would detect all tagged syringes, regardless of where they started. In addition, it reflects the actual bahviour of those anaesthetists who moved the barcode scanner during the IDAS trials. But it has the disadvantage of being the last possible point for confirming that the correct drug has been selected. It is also possible for the electromagnetic radiation (EMR) emitted by an RFID reader to interfere with sensitive medical electronic devices such as pacemakers (Irnich, 2002). With IDASs focus on patient safety, it was decided that the prototype system would use an RFID reader placed on the drug trolley, under the drug tray. 4.4 Associating a DIN with an RFID Tag and Passing it to IDASA simple software application, Associator, was developed to associate a DIN with an RFID tag. It accepts an RFID tag number from a reader, and a DIN from the keyboard or a barcode scanner. The combination is written to a database record. If an RFID tag reader/writer is used, the DIN can also be written to the tag itself. A second application, Operator, was developed to read a tag and retrieve the associated DIN. It polls the RFID reader under the drug tray every half-second, receiving a list of RFID tag numbers. When a tag number disappears from the list, this is taken as a sign that a syringe has been removed from the tray. Operator looks up the database populated by Associator, and retrieves the corresponding DIN. The IDAS software expects input from a barcode scanner attached to a serial port. Operators output is therefore channeled through Eltima Softwares Virtual Serial Port Developer application to make it appear to the IDAS software as though it comes from a serial port. The prototype system was demonstrated to Merry and his colleagues at Auckland Hospital. They seemed confident that RFID technology could functionally replace barcodes in the IDAS system, and raised a number of issues that they believed should be addressed in the next stage of development. 5. OUTSTANDING ISSUESThe prototype system experienced problems detecting syringes in certain conditions. Showing information from the existing barcode labels on RFID tags also proved difficult. The demonstration was not conducted in a live operating theatre so did not experience any EMR interference. However, this needs to be considered. 5.1 Undetected Syringes and Inadvertent ReadsThe drug trays used by in the IDAS system are 25cm wide. As table 1 indicates, an RFID reader placed under the middle of a tray would not be able to read small syringes placed on the edge of the tray. One solution is to rely on RFID readers at the patient. The disadvantages of this have already been noted in section 4.3. Another solution is to use two RFID readers to cover a tray. However, this would require careful placement and synchronization to avoid the reader collision problem (Engels & Sarma, 2002). A third solution is to experiment with types of RFID reader other than the pad style used in the prototype. Gate- and loop-style readers offer a greater read range, but at greater expense. The possibility of the opposite problem, inadvertent reading, was also raised. This might occur where the anaesthetist removes a tagged syringe from the readers range, but not to inject it. For example, the anaesthetist may be moving the syringe to another part of the drug tray, or placing it in the waste bin. Excessive inadvertent reading might in fact lower the usability of the system, as the anaesthetist would have to manually remove the supposed injections from the automated record. Determining the actual incidence of inadvertent reading would best be done through usability trials, with anaesthetists using the Operator application in some simulated operations. If it does present a problem, the syringe movement scenario could be countered by requiring that a syringe is removed for a certain length of time before it is considered removed. A syringe disposal could be correctly identified by having an additional reader located on the waste bin. 5.2 Printing on RFID TagsAs noted in section 3, some information from the current barcode labels must be visible on any RFID tags that replace them. For the demonstration, the barcode labels were simply attached to the RFID labels, and the combined label attached to the syringe. However, to reduce the effort involved in preparing syringes it would be preferable to have a single label. Combination RFID-encoder / barcode printers are available (Collins, 2004b), but do not appear to be suitable as they cant produce the colours required by the standard. There are label printing bureaux that may produce suitable labels, but they are only economical in print runs of hundreds of thousands. 5.3 Electromagnetic Radiation and InterferenceAs noted in section 4.3, the EMR emitted by RFID readers may affect pacemakers. There are also questions on how prolonged exposure to EMR might affect patients. There is a good deal of research on the effects of EMR on people. However, it is not conclusive, and tends to focus on EMR from mobile phones which operate at frequencies higher than 13.56 MHz. On the basis of documentation for the RFID reader used in the prototype, it appears that it does comply with the New Zealand standard (Ministry for the Environment & Ministry of Health, 2000). They anaesthetists pointed out that in a live operating theatre, there are a number of devices known to produce high levels of EMR. The greatest risk appears to be surgical diathermy machines. Nominally, they operate in the 1MHz frequency, but emit so much power that they produce interference harmonics at much higher frequencies (Bassen, 2002). This interference could drown out the relatively low-power transmissions of RFID readers. Experiments in a live theatre situation would be required to determine the actual effect. 6. CONCLUSIONAdverse drug events are costly, both in lives and scarce health care resources. BCMA systems, such as IDAS, are one solution to reducing their incidence and impact. However, barcode scanning appears to disrupt the natural anaesthetic workflow, possibly compromising the effectiveness of BCMA. The prototype system developed in this constructivist research project demonstrates that RFID technology offers the potential to functionally replace barcodes, with minimal disruption to natural workflow. A review of RFID application case studies indicates that RFID tags and readers operating at 13.56 MHz appear to offer a read range and interference profile that makes them the most suitable for location-based systems such as BCMA. Experiments with different sized tags and syringes suggest that the best balance of read range and usability results from smaller RFID tags wrapped around syringes. The development of the prototype system illustrates a number of challenges in working with RFID in the hospital environment. The appropriate choice, and carefully designed layout, of RFID readers is necessary to minimise both undetected tags and inadvertent reading. Some aspects of barcode labels are difficult to reproduce with RFID tags. And the effects of EMR from RFID readers, and on readers from other devices, must be considered. ReferencesAnderson, J. G., Jay, S. J., Anderson, M., & Hunt, T. J. (2002). Evaluating the Capability of Information Technology to Prevent Adverse Drug Events: A Computer Simulation Approach. Journal of the American Medical Informatics Association, 9(5), 479-490. Anderson, J. G., Jay, S. J., Anderson, M., & Hunt, T. J. (2003). Evaluating the Impact of Information Technology on Medication Errors: A Simulation. Journal of the American Medical Informatics Association, 10(3), 292-293. Anonymous. (2003). Smart Healthcare 2003: Conference Review. Retrieved November 1, 2004, from www.idtechex.com Bassen, H. (2002). Electromagnetic Interference of Medical Devices and Implications for Patient Safety. International Journal of Bioelectromagnetism, 4(2), 169-172. Bates, D. W., Cullen, D. J., & Laird, N. (1995). Incidence of Adverse Drug Events and Potential Adverse Drug Events. Journal of the American Medical Association, 1995(274), 29-34. Berger, R. G., & Kichak, J. P. (2004). Computerised Physician Order Entry: Helpful or Harmful? Journal of the American Medical Informatics Association, 11(2), 100-103. Broder, C. (2004). Hospitals Wade into Asset-Tracking Technology. Retrieved October 30, 2004, from www.ihealthbeat.com Brooks, A. (2003). Robot fills prescriptions at UHS. Retrieved October 21, 2004, from www.news.harvard.edu Chassin, M. R. (1998). Is healthcare ready for sigma six quality. Milbank Quarterly, 76(4). Chen, S. C. Q., & Thomas, V. (2001). Optimization of Inductive RFID Technology. Paper presented at the IEEE International Symposium on Electronics and the Environment, Denver, Colorado. Collins, J. (2004a). Healthy RFID Rivalry for Hospitals. Retrieved September 9, 2004, from www.rfidjournal.com Collins, J. (2004b). Label Printer for the Undecided. Retrieved August 1, 2004, from www.rfidjournal.com Collins, J. (2004c). RFID Remedy for Medical Errors. Retrieved June 1, 2004, from www.rfidjournal.com Cornford, T., & Smithson, S. (1996). Project Research in Information Systems. New York: Palgrave. Davis, P., Lay-Yee, R., Briant, R., Ali, W., Scott, A., & Schug, S. (2003). Adverse events in New Zealand public hospitals II: preventability and clinical context. New Zealand Medical Journal, 116(1183). Engels, D., & Sarma, S. (2002). The Reader Collision Problem. Paper presented at the International Conference on Systems, Man and Cybernetics, Hammamet, Tunisia. Food & Drug Administration. (2004). 2002N-0204: Bar Code Label Requirements for Human Drug Products and Biological Products; Final Rule. Retrieved October 21, 2004, from www.fda.gov Foster, P. R., & Burberry, R. A. (1999). Antenna Problems in RFID Systems. Paper presented at the IEE Colloquium on RFID Technology. Irnich, W. (2002). Electronic Security Systems and Active Implantable Medical Devices. Journal of Pacing and Clinical Electrophysiology, 25(8), 1235-1258. Jensen, L. S., Merry, A., Webster, C., Weller, J., & Larsson, L. (2004). Evidence-based strategies for preventing drug administration errors during anaesthesia. Anaesthesia, 59, 493-504. Johnson, J. A., & Bootman, J. L. (1995). Drug-related Morbidity and Mortality: A Cost of Illness Model. Archives of Internal Medicine, 155, 1949-1956. Joint Commission on Accreditation of Healthcare Organisations. (2004). National Patient Safety Goals. Retrieved October 21, 2004, from www.jcaho.org Merry, A., & Webster, C. (2004). Bar Codes and the Reduction of Drug Administration Error in Anesthesia. In press . Merry, A., Webster, C., & Mathew, D. (2001). A New, Safety-Oriented, Integrated Drug Administration and Automated Anesthesia Record System. Anesthesia & Analgesia, 93 , 385-390. Merry, A., Webster, C., Weller, J., Henderson, S., & Robinson, B. (2002). Evaluation in an anaesthetic simulator of a prototype of a new drug administration system designed to reduce error. Anaesthesia, 57 , 256-263. Ministry for the Environment, & Ministry of Health. (2000). National guidelines for managing the effects of radiofrequency transmitters . Wellington: Ministry for the Environment. Nunamaker, J. F., Chen, M., & Purdin, T. P. M. (1991). ystems Development in Information Systems Research. Journal of Managment Information Systems, 7 (3), 89-106. Pappu, M., Singhal, R., & Zoghi, B. (2004). RFID in Hospitals: Issues and Solutions . Retrieved October 21, 2004, from www.rfidjournal.com Patterson, E. S., Cook, R. L., & Render, M. L. (2002). Improving Patient Safety by Identifying Side Effects from Introducing Bar Coding in Medication Administration. Journal of the American Medical Informatics Association, 9 (5), 540-553. Safer Sleep Ltd. (2002a). IDAS Barcoded Ampoules. Safer Sleep Ltd. (2002b). IDAS Syringe Tray. Standards New Zealand. (1996). User-applied labels for use on syringes containing drugs used during anaesthesia (AS/NZS 4375:1996) . Wellington: Standards New Zealand. Walker, J., Spivey Overby, C., Mendelsohn, T., & Wilson, C. P. (2003). What You Need to Know About RFID in 2004 . Retrieved February 9, 2004, from www.forrester.com . Webster, C. (2004). Personal communication with author. Webster, C., Merry, A., Gander, P. H., & Mann, N. K. (2004). A prospective, randomised clinical evaluation of a new safety-orientated injectable drug administration system in comparison with conventional methods. Anaesthesia, 59 , 80-87. Wilson, R. M., Runciman, W. B., Gibberd, R. W., Harrison, B. T., Newby, L., & Hamilton, J. (1995). The quality in Australian health care study. Medical Journal of Australia, 163 , 458-471. Copyright © 2005 Bryan Houliston |
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||
|
Copyright © 2005 NACCQ,
Krassie Petrova, Michael Verhaart & Christo Potgieter. All rights reserved. |
|||||||||||||||||||||||||||||||||||||||||||||||||