|
Bulletin of Applied Computing and Information Technology |
Directions (Research-in-Progress) D1:Use of virtual environments and the selection of measurement parameters for the treatment of phobias |
|
06:01 |
|||||||||||||||||||||||||
Mauricio Plazas Torres Torres, M. P. (2008). Use of virtual environments and the selection of measurement parameters for the treatment of phobias. Bulletin of Applied Computing and Information Technology, 6(1). Retrieved March 14, 2012 from http://www.naccq.ac.nz/bacit/0601/2008Torres_VirtualReality.htm AbstractMedical personnel evaluate patients suffering from phobias without having absolute control of the variables of measurement that might affect the condition or its degree of intensity over time. Identifying metrics that could better quantify current and changing levels of phobias would be of benefit to a doctor. This study focuses on measurement of vital signs of people in a relaxed environment and comparing them with equivalent measures when the person is placed in a virtual reality environment. The purpose of the study is to determine if the changed environment has any influence on the vital signs that are measured. KeywordsVirtual environments, treatment of phobias 1. INTRODUCTIONThe number of phobias and people who suffer from them are increasing due to the stress levels inherent in daily activities. Identification and treatment of these phobias by direct exposure to the situation or activity causing the phobia can be dangerous to the physical and psychological health of the patient (APA - American Psychiatric Association, 2000). An increase in patient trauma or physical harm may result from such exposure to the situation or activity that is at the centre of the patient’s phobia. Virtual reality technologies have been used to reduce the levels of trauma caused to the patient, obviating the need for the patient to actually experience the phobia in the clinical conditions (Waterworth, 1999) (Figure 1). Figure 1. Medical Center for Phobia Treatment: Mary Levin, University of Washington. Virtual reality has been used extensively in technological research (Rosen, et al, 1996). Applying these techniques to the treatment of phobias may allow a patient to experience a specific phobia such as a fear of enclosed spaces, a fear of heights or a fear of driving a car, in a more controlled environment, with the opportunity to quickly and safely revert to a relaxed environment to avoid dangerous psychological reactions (Riva, 2005). Two immediate questions arise:
Methods to assess phobic reaction levels involving direct exposure to the conditions that cause the phobia can cause both physical and psychological damage to the patient. Virtual reality equipment such as infrared tracking and a Head Mounted Display (Scherer, 1977) (Figure 2) are used to create the virtual environments used in research such as this. Other equipment is used to measure the reactions of the patient, including cardiac frequency meter, software for processing the frequency of the voice and a thermographic camera. The virtual environment that is created is projected in the Head Mounted Display for the patient to experience. Figure 2. Virtual Reality Equipment Surveys are the currently accepted method to measure the degree of phobic reaction and the effectiveness of treatment for phobias (APA - American Psychiatric Association, 2000). This research proposes the use of a more quantitative assessment methodology, less reliant upon the patient’s perceptions, providing a comparative scale against which to assess the level of phobic reactions (Cohen, 1977). The key feature of the proposed assessment methodology is measurement of changes to corporal vital signs, proven by medical specialists to be affected with changes in stress levels. This research identifies and measures specific vital signs of a person in a relaxed ‘rest’ environment, a natural environment will minimal stress imposition. It then compares the results to similar measurements taken while experiencing a virtual environment that simulates exposure to the phobias to be examined. The particular vital signs measured in this research are cardiac frequency and corporal temperature. Another measure used is the fundamental frequency of the person’s voice, measured using free software for voice processing (SPS - Speech Filing System, 2008). The aim of the project is to develop a means of quantifying the changes brought about by the virtual environment on the patient’s stress levels without the use of the traditional, less-than-objective methodologies. The phobias selected for inclusion in this project are claustrophobia (a fear of being locked in or enclosed) and acrophobia (a fear of heights). 2. METHODOLOGY2.1 Ethical and Safety ConsiderationsEthical and safety considerations are necessary for any research project where processes may have potential effects on the people involved in the research. Medical experts with expertise in the area of vital signs were consulted prior to undertaking this project. The recommendations arising from these discussions were:
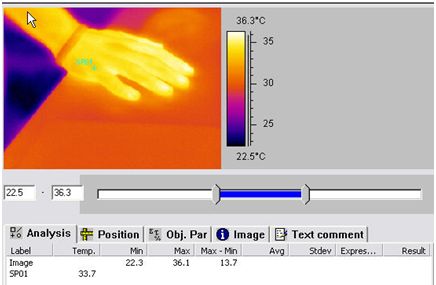
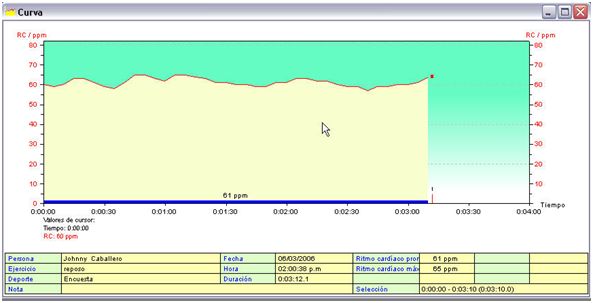
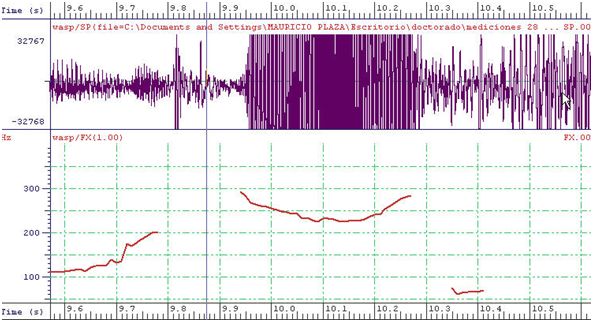
2.2 Vital SignsSome elements to be monitored, such as the frequency of heart beat, cardiac variability, patient temperature and the fundamental frequency of the patient’s voice, will provide quantitative measures of the patient’s stress levels. These measures can also identify changes in the patient’s reactions relating to a specific phobia. The vital signs selected for measurement in this project were determined by the relative magnitude of change when stress levels are modified. Other vital signs considered for inclusion lack evidence of correlation to stress levels in medical literature. 2.3 Stress Levels and the Regulation of TemperatureIntense stress produces emotional changes in a patient that leads to poor temperature regulation in the body. Parts of the body with high capillary irrigation, such as the hands, exhibit higher levels of temperature change. The temperature change comes about because of hormone segregation causing blood vessel constriction, muscular spasms of the walls of the arteries and oxidation of the red cellular membranes, leading to thickening and clot formation due to the platelets (Ali, 2002). Thermographic tests of the hand do not demonstrate a large enough level of temperature change to identify differences between control patients and the two groups with phobias in the virtual environments (Figure 3). Figure 3. Thermographic Data 2.4 Heart Rate VariabilityHeart rate variability refers to arrhythmia, a non-symmetrical rhythm of the sinusal node, the heart’s ‘pacemaker’ (McCraty, et al., 1995) occurring during the breathing phase. A person’s emotional changes influence this arrhythmia (Hall, 2004). Measuring heart rate variability rather than cardiac frequency (Figure 4) reveals a significant reduction that correlates to the exposure to the virtual environments. Figure 4. Cardiac Frequency (Rest Environment) 2.5 Fundamental Frequency of the VoiceThe muscles of the human body, including the vocal cords, vibrate at a specific frequency. Stress can cause changes to this muscular vibration frequency and to voice frequency. A useful measure is the fundamental frequency of the voice, the frequency of the sound produced by the vocal cords. This is highly correlated with intonation and stress levels. The two environments involved in this project, the natural/rest and the virtual environments, can be distinguished by changes in the fundamental frequency of the voice by measuring average values (Scherer, 1977). Neither voice duration nor volume demonstrate any changes that could be correlated with the specific environment involved, so are not considered useful parameters for measurement (Figure 5). Figure 5. Voice Register, Fundamental Frequency and Energy 3. EXPERIMENTAL PROCEDUREVirtual environments to simulate claustrophobic and acrophobia experiences were created for use in this research. Vital signs of participants in the study were measured in a naturally relaxed (rest) environment to compare with results obtained when exposed to the two virtual environments. The project attempted to determine if these virtual environments produced similar effects to real world experiences, thus enabling their use as a tool in the treatment of the phobias. Participants for the study were selected from engineering students from the Universidad Libre, Bogot�, Columbia (ULC). The number of participants needed was statistically determined as 308 of the 1,350 students at the ULC, providing significance at the 0.015 level, with a probability of change of the average value of 90%. 43% of the participants reported prior experience of some form of phobia, with the remaining 53% reporting no phobias. Of the participants with phobias, 56% identified as suffering from acrophobia, 18% from claustrophobia and the remainder from other phobias. The project was carried out as follows:
4. RESULTSSome of the vital signs did not show significant differences with the differing environments. Others, however, provided enough differentiation that they could be useful in determining changes that may occur during the treatment for a phobia. Further, there are indications that the specific virtual environment to which the patient is being exposed (claustrophobic or acrophobic) can be identified solely through the data collected. Of the participants who had identified as suffering from acrophobia, 47% reported that they were mildly affected by the virtual environment. Only 5% reported feeling ‘very affected’. Improvements to the virtual reality experience are necessary before there could be any valid comparisons to the ‘real’ experience. Of participants 8.8% reported feeling sick either during or immediately after experiencing the virtual environments. These symptoms, described as “motion sickness” or “simulation sickness”, are caused by a discrepancy between brain and senses responses. Even with the virtual environments, a participant is still able to perceive some aspects of the real world beyond the virtual, and the differences lead to these feelings of sickness. There was no significant difference in cardiac frequency measurements for individuals experiencing the claustrophobia virtual environment (rest environment: 83.3bpm, virtual environment: 84.4bpm, giving ANOVA significance of 0.754). Average cardiac frequency cannot be used to identify patients who would be affected by the virtual reality conditions. The same applies for the acrophobia virtual environment, which had an ANOVA significance of 0.413 - there was no statistical difference in cardiac frequencies between rest and the two virtual reality environments. For participants suffering from acrophobia, average body temperature showed significant change from the rest environment. The same was not true for those suffering claustrophobia; ANOVA significance of 0.558 would indicate that body temperature changes are not a good indicator for this condition. The change in temperature for those with claustrophobia was in fact very small:
Table 1. Change in Body Temperature The change in body temperature for participants appears to differ from that which would be expected from the existing medical literature. Most studies report a drop in body temperature when undergoing stress. It is possible that while the reaction to the virtual environment is not very strong, the experience of the phobia itself causes an increase in the participant’s general levels of attention. This increased attention may generate the same increase in body temperature that would normally be associated with a relaxed environment. Participants with acrophobic tendencies had significantly higher fundamental voice frequencies compared to rest environment measurements. The energy of the voice did not differ significantly between the three environments, and so is not a useful measure to determine the impact of the virtual environments, as shown in the table below.
Table 2. Change in Energy (Voice) There was a significant difference in cardiac variability between the “at rest” and the combined measurements of the virtual environments, with ANOVA significance lower than 0.005, with a decrease in the virtual environments that is supported by the existing medical literature.
Table 3. Change in Cardiac Variability Cardiac variability is the only measure that provided an effective means of identifying the level of stress generated by either virtual environment. The other vital signs were only able to identify changes in the acrophobia virtual environment. These results indicate that the claustrophobia virtual environment does not provide an equivalent experience to that of the real environment. 5. CONCLUSION Figure 6. Virtual Reality Center Virtual reality tools are used in the treatment of phobias by some medical centres (Zajtchuk, et al, 1997) (Figure 6). The aim of this research project was to identify specific vital signs that could be used as an objective and quantifiable measure of effectiveness of the treatments involved Average cardiac frequency, and the energy and duration of the voice were not useful measures to identify the reaction to the virtual environments involved in this study. Other measurements such as body temperature, cardiac variability and fundamental frequency of the voice were able to distinguish between the natural/“at rest” and the virtual environments. Only cardiac variability could be used to measure both claustrophobic and acrophobic virtual environments. Body temperature and fundamental frequency of the voice were only able to distinguish between natural/“at rest” and the acrophobic virtual environment. 6. ACKNOWLEDGEMENTThe authors acknowledges with thanks the support provided by BACIT editorial team. RERERENCESAli, M. (2002), “Temperature dysregulation in stress”, Retrieved December 31, 2008 from http://www.majidali.com/temperat.htm APA - American Psychiatric Association (2000), Diagnostic and Statistical Manual of Mental Disorders DSM-IV TR, 4th Edition, American Psychiatric Publishing, 943 p. Cohen, D.C. (1977), “Comparison of self-report and overt-behavioral procedures for assessing acrophobia”, Behavior Therapy, v. 8, n. 1, p. 17-23. Emmelkamp, P.M.G., Krijn, M., Hulsbosch, A.M., de Vries, S., Schuemie, M.J., van der Mast, C.A. (2002), “Virtual reality treatment versus exposure in vivo: a comparative evaluation in acrophobia”, Behaviour Research and Therapy, v. 40, n. 5, p. 509-516. Hall, M., Vasko, R., Buysse, D., Ombao, H., Chen, Q., Cashmere, J.D., Kupfer, D., Thayer, J.F. (2004), “Acute stress affects heart rate variability during sleep”, Psychosomatic Medicine, v. 66, n. 6, p. 974-976. McCraty, R., Atkinson, M., Tiller, W.A., Rein, G., Watkins, A.D. (1995). “The effects of emotions on short-term power spectrum analysis of heart rate variability”, The American Journal of Cardiology, v. 76, n. 14, p. 1089-1093. Riva, G. (2005), “Virtual reality in psychotherapy: review”, Cyberpsychology & Behavior, v. 8, n. 3, p. 220-230. Rosen, J.M., Soltanian, H., Redett, R.J., Laub, D.R. (1996), “Evolution of virtual reality [Medicine]”, Engineering in Medicine and Biology Magazine, IEEE, v. 15, n. 2, p. 16-22. Scherer, K.R. (1977), “Effect of stress on fundamental frequency of the voice”, Journal of the Acoustical Society of America, v. 62, suppl. n. 1, p. S25. SPS - Speech Filing System (2008), “Tools for Speech Research”, Department of Phonetics & Linguistics, University College London, In: www.phon.ucl.ac.uk/resource/sfs. Waterworth, J.A. (1999), “Virtual reality in medicine: a survey of the state of the art”, Retrieved December 31, 2008 from www.informatik.umu.se/~iwworth/medpage.html. Zajtchuk, R., Satava, R.M. (1997), “Medical applications of virtual reality”, Communications of the ACM, v. 40, n. 9, p. 63-64. Home | Issue Index | About BACIT
| |||||||||||||||||||||||||||